The Nature of Drugs by Alexander ‘Sasha’ Shulgin gives you a peek into the awesome lecture series that Sasha gave in the late ’80s. The lectures give an overview of how the body works and how drugs (including psychedelics) influence it. Throughout the book, you are greeted with the positive attitude and joking demeanour of Sasha, as well as poignant criticism of drug laws that would still apply today.
A review copy was graciously provided by Synergetic Press.
If you want to help preserve the legacy of the Shulgins, please consider donating to the Shulgin Foundation. The nonprofit organisation is dedicated to preserving the legacy and work of Ann and Sasha Shulgin. They are committed to carrying forward their values by promoting education, research, and harm reduction around psychedelics and psychoactive substances while fostering community and connection.
Summary Review of The Nature of Drugs

Author: Floris Wolswijk is the founder of Blossom. He started Blossom in 2019 to help translate psychedelic research to a broader audience. Since then, he has grown the database to encompass 2000 papers and hundreds of other valuable resources. Floris has an MSc in Psychology and offers psychedelic-assisted coaching at FLO.
Introduction
The lecture series presented here is the first semester of Sasha’s introduction to pharmacology. The lectures were given in a time of moral panic, when the average person was vehemently against all drugs, not nowadays when mainstream newspapers are touting the benefits of MDMA-assisted therapy. This alone makes the lecture series a unicum in that time period, a place where rational discussion could take place about how drugs worked.
As many more nowadays also promote (e.g. Carl Hart), Sasha knew that for most people, drug use is something positive. Most drug users don’t become abusers or addicts. What the world needed then and now is more information, not scaremongering. The lecture series provided just that, factual information that others could use to make more informed decisions.
Maybe most important is Sasha’s stance towards new information. Instead of ‘proving’ something is so, which may still be the prevailing stance in science, he argues that we should look to disprove (falsify) previously held hypotheses. Or in other words, it’s impossible to do an experiment that proves a hypothesis (i.e. he was a Popperian). More on this in lecture 8.
This first of three parts lecture series covers, in the words of editor Keeper Trout: “How a drug gets into the body, how it moves around, what it does, what happens to it, and how it gets out. In doing so, Sasha attempts, as he puts it, to present “what can be bad about drugs, and what is sometimes very good about drugs. Warts and all.” “
Lecture 1 – Course Introduction
The recommended reading for the lecture is Chocolate to Morphine by Andrew Weil, a book that describes a lot of different compounds and how they influence the body. The book, and the lectures, give an honest overview, presenting them with “warts and all“.
Drugs are all around us. Not only those recognized widely as drugs but also compounds such as caffeine, nicotine, and alcohol. And if we look beyond what many people consume, this also includes things such as psychoactive nuts (e.g. betel nuts). What we want to know about each of them is their 1) actions, 2) risks, and 3) virtues.
Sasha doesn’t like to use the word addiction. He thinks it’s better to describe it as someone having a bad relationship with a drug. Drug abuse then is defined as someone having a dependency on a drug. Though he has used over 150 different (mostly psychedelic) compounds, he isn’t abusing any of them. What he does have a bad relationship with is smoking, and because he knows he can’t have a good one, he doesn’t smoke anymore.
Speaking with the knowledge of someone way ahead of his time, Sasha also notes how a lot of the diseases we are currently facing “actually stem from something upstairs in the head.” Here he also remarks on the power our perception of reality has on the world. The ‘facts’ may be the same for different people, but the actions they take as a result may differ significantly. Here he also argues (as he will throughout the lecture series) that remaining in control of your own choices is paramount towards living the good life. “To choose vice is better than having virtue chosen for you.”
So, what are drugs? Some would say it’s compounds that change your perception. But will that then also include aspirin or even water? And if we go even broader, could it not also include placebo’s as they can sometimes be as ‘strong’ as the actual drug. Looking at the FDA definition, drugs are defined more narrowly and exclude foods and medical devices. Finally, Sasha settles on the following definition of drugs: “A drug is something that modifies the expected state of a living thing.”
If we investigate what drug abuse is, we have to look at what, who, where and how. It’s easiest, especially for drug enforcement, to look at what. Just ban a substance and get on with it. But this forgets the other elements, as any ‘drug’ can be abused (e.g. drinking 8 litres of water in one sitting will do you no good). Who uses or prescribes a drug is also seen as a differentiator of the badness of a drug. Ketamine prescribed by a doctor is usually seen as virtuous, taking it for pleasure as abuse.
Finally, we settle on the definition also used by Weil, that “drug abuse has nothing to do either with the legal or medical approval or disapproval of the drugs involved or with the reasons for their use. Any use of a drug that impairs physical or mental health, that interferes with one’s social functioning or productivity is drug abuse.” To that, I would add that one would look at this over a period of time (e.g. a month) instead of investigating one’s productivity whilst enjoying a tab of LSD.
The lecture ends with a few different terms:
- Habituation: Repeated use without serious harmful effects
- Addiction: Not used much in medical circles, but implying negative effects of repeated drug use
- Dependence: Conditioned pattern of drug-seeking behaviour through repeated use
- Physical dependence: Neural or metabolic changes to better accommodate a drug (influencing tolerance and/or withdrawal)
- Psychological dependence: Positive psychic response that leads to repeated use
- Relapse: Return to level of drug use that is agreed upon to be bad/harmful
- Craving: Intense desire or obsession for a drug (even years after stopping)
- Tolerance: Decreased response to same amount of drug (acute & chronic)
- Withdrawal: Effects when stoping a drug one is dependent on (e.g. hangover, rationalizing why to continue, seeking alternatives)
Lecture 3 – The Origin of Drugs
Note: Part of the recording of lecture 2 is missing, so notes from this lecture are intertwined with the first and fourth lectures.
How drugs have come about and how we discovered and used them as humans are covered in this lecture, as well as the ways they interact with the laws and how those are formed.
Why some drugs are illegal (e.g. heroin) and others not (e.g. methadone) doesn’t always (or nearly never) has any rational grounds. But undoing a law would require the acknowledgement that it was made in error, not something that governments do easily.
Every culture has discovered drugs, and broadly they can be categorized as those that numb (downers) and excite (uppers). When a new plant (drug) enters into another culture, it has almost always been rejected. This is true of tobacco, coffee, and just about any drug introduced through the mixing of cultures.
This rejection of drugs took on a more serious character at the turn of the 20th century, which intensified through the 1960s and culminated in the formation of the drug schedules (still in use today). In 1970 the Controlled Substance Act passed, which still classifies most psychedelics as one of the worst drugs (high potential for abuse and without accepted medical use). Around this time, the narrative changes from a drug (ab)use as a concern for taxation to become a criminal offence, with all subsequent consequences.
The Emergency Scheduling Act of 1984 added to this and allowed drugs to be scheduled without a hearing period. This is how MDMA originally got scheduled, and after some back and forth, it was eventually made illegal by the ‘proper procedure’. And following this, the Controlled Substance Analogues Enforcement Act (also known as the Designer Drug Bill), passed in 1968, also made it easier to ban drugs that were similar (analogues) to other banned substances. A drug only needs to be ‘substantially’ similar in structure, though the term is vague enough to encompass any compound.
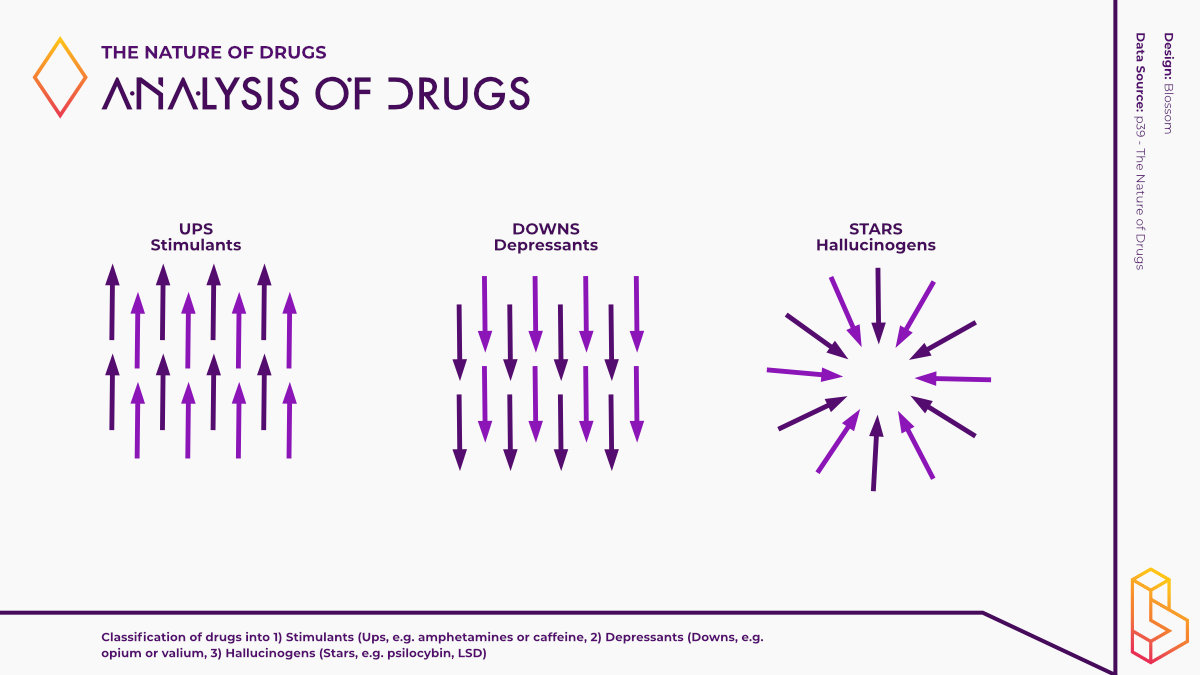
Discussed in the context of the drug laws, Sasha notes that drugs can be classified into three different groups. A reference book by the same name groups them in Ups, Downs, and Stars. Ups are stimulants, Downs are depressants, and Stars are hallucinogenic.
Lecture 4 – The Plumbing of the Human Body
Imagine the body to be a one-meter long pipe, some things go in via the mouth, and some other things come out the other end. That is in essence what the body is, a processor of inputs (which can include other ways than the mouth) which then outputs other things, mainly waste products. Along the route, we meet the stomach, small intestine, big intestines, colon, rectum, and anus. For a drug to have an effect, it needs to be absorbed/processed (get in the blood) somewhere along this route.
The motion of drugs is called pharmacokinetic: pharmaco- (drugs) -kinetics (movement). The action of drugs is called pharmacodynamics: pharmaco- (drugs) -dynamics (action). Pharmacokinetics looks at the plumbing and measures the levels of a drug, how it gets processed, and finally removed. Pharmacodynamics investigates the relationship between the drug and the effects it has (on the body and mind).
Your body doesn’t know a drug from a food (molecule), the body takes it in and through the whole process, gets rid of it somewhere. This means that most of a drug will not get to the specific area where it has an effect. Sasha argues that often 99% of a drug will get lost this way (some drugs are the exception, they seek out the specific receptors to bind to, e.g. iodine will seek out the thyroid).
A human has about 5 to 6 litres of blood which gets pumped around the body about once every minute. If a drug is injected, this can be done by either slow infusion (over a period of time) or as a bolus (giving it all at once, which slowly diffuses over the whole blood supply, this takes about 2-3 minutes).
If a drug is absorbed at the very start of the pipe, in the mouth, this is called sublingual (under the tongue) absorption. It is taken through the mouth directly into the blood supply. This can be done to bypass the (filters of) the stomach/gut (e.g. taking DMT orally without any other substances will not give you hallucinogenic effects).
Another route taking place at the head is insufflation or snorting. The same principle applies here, the small blood vesicles in the nose absorb the drug. Other routes discussed by Sasha are 1) subcutaneous (under the skin), 2) intravenous (in the vein), 3) suppositories (rectally), 4) inhalation (mostly lungs), 5) intramuscular (into the muscle), 6) intraperitoneal (around intestines), 7) trepanning (in the brain).
If a drug is taken via the mouth, most of the absorption won’t happen until it has passed the stomach. Though the contents of the stomach, effectively blocking something from going to the small intestine, can severely affect the rate of absorption of a drug. One reason why drugs don’t get absorbed in the stomach is that the environment is quite acidic, whilst most drugs are basic (the opposite of acidic). Once in the small intestine, many drugs get ‘transported’ through the hepatic portal system (taking blood from the intestines to the liver). About a third of the heart’s energy is dedicated to moving blood around here, which results in about 1,5 litres flowing through it every minute.
The effects of drugs that bypass the stomach are stronger (per the same dose) because only about 30% of the drugs make it through the liver’s filter. This doesn’t mean that the liver only filters out drugs. It could even be so that the liver turns an inactive version of a drug into a biologically active one. Drugs that are not active themselves (that have no intrinsic activity) and turn into the active versions are called prodrugs (although Sasha would prefer to call them predrugs – psilocybin is the prodrug of psilocin).
Changing a drug (molecule) into something else can be called biotransformation (and was called metabolism or detoxification, but the process could just as well lead to the toxification of something non-toxic). One rule of thumb, when thinking about the liver, is that it tries to make things more (water) soluble. The more effortless something dissolves in water, the easier the body gets rid of it, the fattier/oilier, the longer it stays/is active.
This concept of getting rid of drugs also applies to the half-life of a drug. Over time, a drug is removed from the different parts of the body. Interestingly, this is also why some drugs are still visible on tests over a long period (days/weeks) (as the fatty tissues release them very slowly, so a small percentage remains noticeable). And this is also why many drugs are removed quickly from the bloodstream but remain active by sticking to receptors (e.g. 5-HT2a (serotonin) receptors) in the brain.
Sasha then switches gears and talks about the higher-level pharmacodynamics, stating that most drugs are very effective in the first 5-10 years, but their effectiveness drops and more side effects will be found after that. He also argues that the placebo effect is a big part of a drug’s action but not a part that should be taken lightly.
Lecture 5 – More Body Plumbing & the Nervous System
This lecture dives deeper into how the body processes drugs. We go back to the example of the bolus. If you introduce a drug suddenly, the body will process it over a given period. The half-life will depend on:
- The size of the bucket (e.g. your blood)
- Rate of entry/exit (i.e. how fast your kidneys clear out a drug – renal clearance)
- But the half-life is independent of the amount of drug introduced
Or, in other words, introducing more or less (without considering some other mitigating factors) of a drug will not make it last longer/shorter (though it can be more intense/have more effects at the tail end).
Drugs (including medications) are usually given based on the subject’s body weight. This is because one expects a larger person to have more receptor sites, though this conventional wisdom doesn’t always hold up. Recent experiments show only a weak or no relationship between bodyweight and the subjective experience of psilocybin (Garcia-Romeu et al., 2021). So, in many cases, the simplest dosing schema is a uniform dose.
Sasha discusses more details about how drugs are metabolised, though I think a lively example will do best to describe how the different administration routes have effects that one would not usually expect: “One trick we used to do in college … we’d run hot water into the sink and really get rolling hot water with steam… Then we’d take a liter of ethanol [alcohol] and throw it in the sink and stick our heads down in there and inhale through our mouths a couple of times. Oh! You are just right there. Into the lungs, into the brain! None of this first-pass metabolism. No first-pass that hits the liver. You’re very quickly roaring drunk, and then it diffuses on through the blood system and gets more or less averaged because you’re getting a bolus to the brain. Once it gets averaged, the average level is too low to be intoxicating and you’re sober about ten, twenty, thirty seconds later, but a little less bored.”
We then move on from the plumbing to the wiring. Here we meet two central concepts, 1) afferent and 2) efferent. Afferent is the direction towards the central nervous system (CNS) (sensory, e.g. teleceptors). Efferent is the direction of nerves and nerve systems going out of the brain/CNS. In the afferent system, some barriers (e.g. your skull) include the blood-brain barrier – which keeps charged things (including many drugs) outside of the brain. The outside world is the periphery or the peripheral nervous system – inside is the CNS.
If we take a look back at the three types of drugs mentioned before, then Downs (ketamine, PCP) block signals from getting in (afferent), whilst Ups (and in a way Stars) add to the incoming signals.
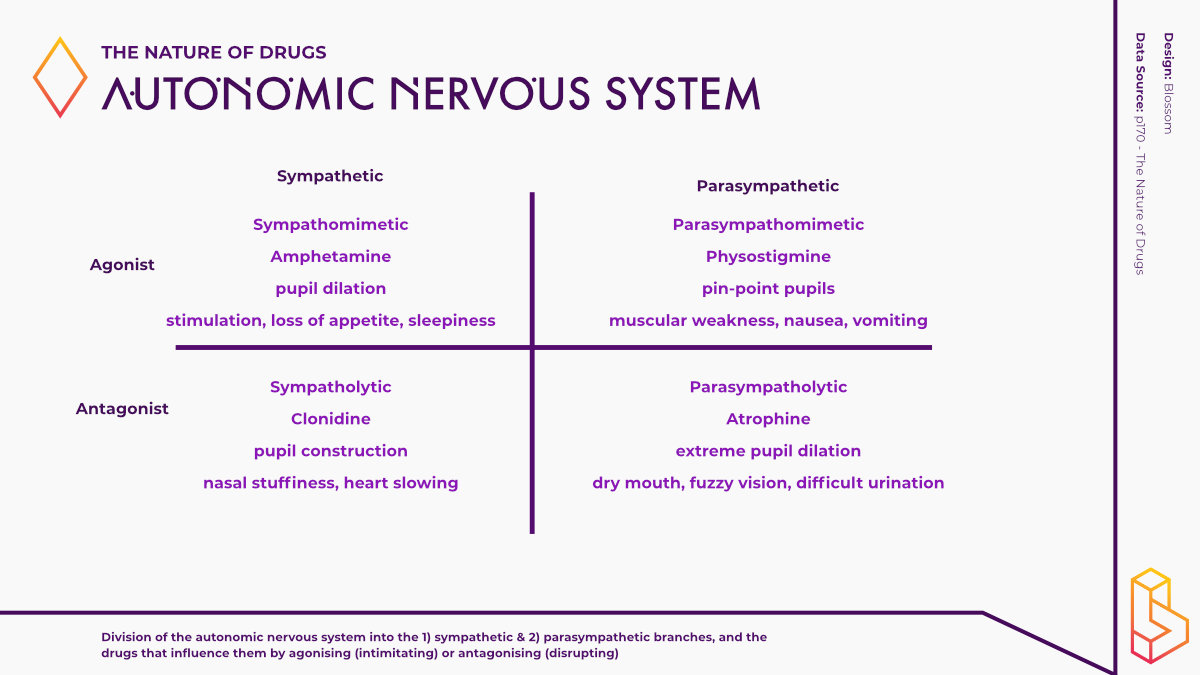
Within the body, you have proprioceptors, signals coming from the muscles, which tell you where each body part is. Interoceptive signals go from other parts (e.g. heart, gut) to the brain. Signals going back from the brain downstairs (efferent) can be both voluntary (e.g. moving your hand) and involuntary (e.g. heart beating faster after scare – autonomic nervous system). The autonomic nervous system is usually on autopilot, but with practice, people can influence it (e.g. make heartbeat go slower, lower blood pressure). Drugs act on the autonomic nervous system.
The autonomic nervous system consists of the sympathetic and parasympathetic branches, both of which keep each other in balance. At both, you can introduce agonists and antagonists, leading to the following division. There are drugs that “imitate the sympathetic nervous system (sympathetic agonists, sympathomimetic agents) and those that inhibit it (sympathetic antagonists, sympatholytic agents). Similarly, there are drugs that imitate the parasympathetic nervous system (parasympathetic agonists, parasympathomimetic agents) and those that inhibit it (parasympathetic antagonists, parasympatholytic agents).”
Lecture 6 – Drug Action
The sixth lecture looks at how drugs influence a person, both at the level of neurons and when looking at a whole person. These two levels of analysis are both valid entry points, and (in my opinion) it’s often missed when one is speaking about one level that it doesn’t invalidate that explanations at the other are also valid.
Sasha states about the first level: “[This approach is] based on the fact that all affective states, from emotion to stimulation to depression to curiosity, are somehow functionally explainable (if not today, at least someday) by the tracing of neuronal pathways, and all these pathways are glued together by the magic of neurotransmitters.”
Looking at the second, holistic level: “[A]ll drugs can be looked upon as being organizing or disorganizing, and they can be looked upon as being directed towards ill people or towards well people.”
When you give multiple drugs to a person (polypharmacy), they interact in unknown ways. Many drugs are tested extensively before going on the market, so we feel safe (you can’t prove it, see lecture 8, but can be confident about it). But, the average number of drugs in a person at the ICU is 16, between which you won’t be able ever to know the ways they will interact.
Two terms for this interaction are 1) potentiation and 2) synergism. Potentiation is when one drug makes another more active without itself having much action. Synergism is when two drugs both have actions that add up to more than the sum of the parts.
An example of synergy is the danger of combining alcohol with barbiturates. But synergy can also be used for positive effects, such as combining two drugs to more effectively treat someone with a lower dose.
The latter part of this lecture describes five categories of drug action as envisioned by Louis Lewin.
- Excitantia: similar to Ups (caffeine, ephedrine, khat)
- Inebriantia: intoxication (alcohol)
- Hypnotica: depressing the CNS (barbiturates, tranquilizers)
- Euphorica: narcotics (morphine, heroin – turn inwards)
- Phantastica: psychedelics or Stars (opposite of euphorica – more aware)
Lecture 7 – Memory & State of Consciousness
If we can say anything about drugs, particularly psychedelics, they change consciousness. Sasha argues that memories are stored forever, though he also mentions amnesia – the ability to forget. Though not elaborated on much further, there is a lot of discussion about what remembering entails. Is it to bring back exactly what had happened before, or is your new re-membering another unique instance of the events that took place? Not to speak of the work of Elizabeth Loftus and others on the ease that we mis-remember or can make up memories when triggered in the right way.
Sasha then moves on to describe the work done by Anton Mesmer, a physician who healed people (back in 1778) with iron wands. Though our current belief is that these wands did nothing by themselves, this is a clear example of the placebo effect, as many of his patients did improve significantly. (for more on Mesner, see these Radiolab and Hidden Brain episodes). Sasha explains it as follows: “I don’t know to what extent it was really his magic or to what extent he had found a vehicle into a person’s own awareness and their own capability of healing themselves. I rather suspect the latter…”
Mesmer – from which the term mesmerizing comes – is a prime example of hypnotism, which Sasha later likes to similar capabilities in shaman. One part of healing this way may not only be giving up choice but giving up your power towards someone else. In the context of explaining conditioned responses, Sasha argues: “Don’t ever forget that the decisions still have to be made.”
The lecture then dives deeper into explaining a case of schizophrenia, “is like a switchboard in which everything is lit up.” But finding a specific biomarker or test has been a disaster, according to Sasha (and recently mirrored by Thomas Insel – saying that advances in neuroscience have yet to benefit patients). “You’ve got to communicate with a person.”
Even defining mental illness is heavily dependent on the context. This context can be cultural (e.g. what level of melancholy is accepted), based on when you’re feeling what emotions (e.g. one week versus one year after losing a loved one), and many other factors.
At the end of the lecture, Sasha warns those who are getting into science: “[D]o not fall in love with the hypothesis… Do not try to prove a hypothesis. Do not design an experiment that will prove your hypothesis, because it cannot be designed… No matter how you design it, no matter how successful your experiments are, it only takes one failure to throw the whole hypothesis out.”
Lecture 8 – Research Methods
According to Sasha, research is about asking questions, and how you ask those questions matters. Questions can be asked in two categories, 1) learning what is already known and 2) creating new knowledge. Sasha laments that people (scientists) are mostly answering the first type of questions. When trying to answer the second type of question, Sasha (channelling his inner Francis Bacon) argues that you want to devise a hypothesis (and alternative hypothesis) and try and disprove it.
For instance, when evaluating the safety of a drug, you can prove that it’s hazardous. But no matter how many tests you do, you can’t prove safety. “So, design something that will tear your hypothesis apart and do the experiment. If doesn’t, cycle around again. If it does, cycle around again. This is a process of inductive or strong inference.”
When working on new drugs, patents can help protect novel discoveries. Sasha identifies two types of patents, 1) ownership of the compound itself and 2) use of a known patent (utility patent). Even back then, Sasha was aware that those claiming patents make them as broad as possible, trying to prevent others from using/infringing on their new discovery. Though the discussion is better left elsewhere, a hot debate is currently ongoing within the psychedelic field surrounding the patenting of (not so) novel compounds.
If a wholly new compound is made, it can be labelled an ‘Investigational New Drug.’ After doing this, it has to go through the four clinical study phases. Along the way, the safety, dosing, and efficacy will be tested. The first phase will test the safety in ‘healthy normals.’ The second phase consists of testing the efficacy in the target population (e.g. those with depression). The third phase takes the trial outside to other doctors and helps build up the statistics needed to approve a drug. Some, not all, drugs require a fourth phase in which they measure real-world efficacy and safety.
The difficulty or exciting thing with psychedelics is that animal tests will give you less information than other drugs. You can learn about relative safety/toxicity. But besides a few indicators (e.g. head-twitch in mice), you are left with very few clues on how humans will respond to a novel psychedelic and its long-term effect without testing it in humans.
For more on that, see our clinical trials database.